
Introduction
- STIs continue to be a major public health challenge in the United States. In fact, the CDC reports that STIs as a whole are at an all-time high.
- The CDC estimates that almost 20 million new infections occur each year—and 50% of these infections occur
in young people between the ages 15 to 24.
- The bacterial species causing STIs have some distinctive characteristics.
- Because these organisms are dependent on sexual intercourse (which might be sporadic) for transmission, The pathogens must:
- Persist in an infective form until that person has sexual intercourse.
- Hide themselves from recognition and elimination by the immune system.
- Be ready to be transmitted when the infected individual has sexual intercourse.
- In this section, we consider the common STIs and the bacterial species that cause: Chlamydial
Chlamydial Urethritis
- Chlamydial urethritis is the most frequently reported STI.
- Chlamydial urethritis represents one of several diseases collectively known as non-gonococcal urethritis, or NGU.
- About 50% of NGUs are due to chlamydial urethritis, 25% to Ureaplasma urethritis, and another 25% are due to unidentified infectious agents.
Causative Agent and Epidemiology
- The disease chlamydia or chlamydial urethritis is caused by Chlamydia trachomatis, an exceptionally small (0.35 μm), round to ovoid-shaped organism.
- Being an obligate, intracellular parasite, it has one of the smallest bacterial genomes, having about 600 genes (Escherichia coli has around 4,200 genes).
- Serotypes D–K of C. trachomatis are associated with NGU.
- C. trachomatis has a biphasic and unique reproductive cycle.
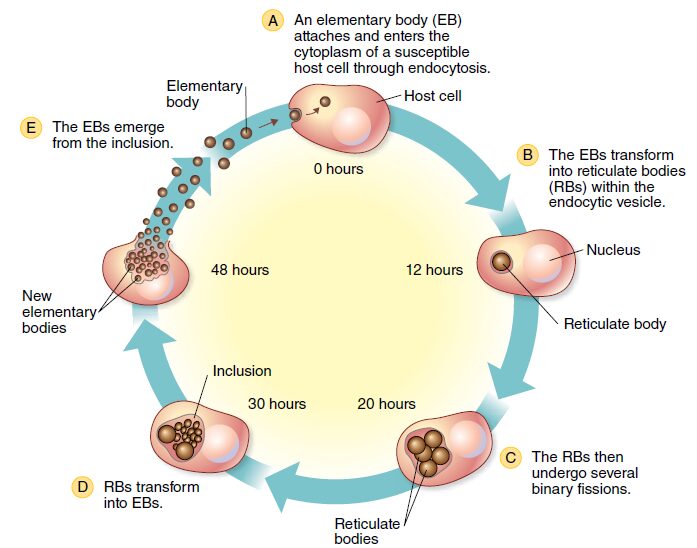
- There is a non-replicating, extracellular, infectious elementary body (EB) and a replicating, intracellular, noninfectious reticulate body.
- Humans appear to be the only host for the organism.

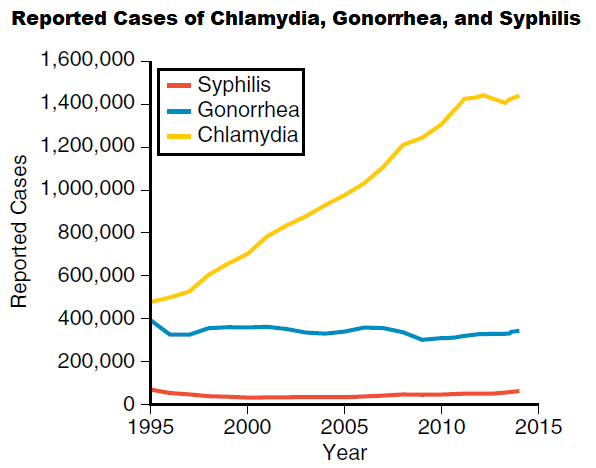
- Chlamydial urethritis is the most common STI globally and the most frequently reported nationally notifiable infectious disease in the United States.

- About 75% of these cases occur in women between 15 and 29 years of age.
- Besides an increase in incidence of chlamydial urethritis, the rise in reported cases is due to the increased number of screening programs available and the development of better diagnostic tests.
Clinical Transmission of chlamydia
- C. trachomatis is transmitted by vaginal, anal, or oral sex.
- In fact, any sexually active individual can be infected through sexual contact with an infected individual.
- The disease has an incubation period of about 1 to 3 weeks.
- Chlamydia often is referred to as the “silent disease” because the organism does not cause extensive tissue injury directly.
- Thus, some 85% to 90% of infected individuals are asymptomatic, whereas others might not seek treatment and thus can unknowingly pass the disease on to others.
- If symptoms do occur, females often note a slight cervical discharge (drainage of fluid from the vaginal wall and cervix), as well as inflammation of the cervix.
- Burning pain also is experienced during urination, reflecting infection in the urethra.
- In complicated cases, the disease can spread to, block, and inflame the fallopian tubes, causing salpingitis.
- About 40% of untreated infections progress to pelvic inflammatory disease (PID), which is an inflammation of the uterus, fallopian tubes, and ovaries.
- PID from chlamydia and gonorrhea is believed to affect about 50,000 women in the United States annually.
- Often, however, there are few symptoms of disease before the salpingitis manifests itself, thus adding to the danger of infertility and a life-threatening ectopic pregnancy, in which a fertilized egg begins to develop in a fallopian tube rather than the uterus.
- In fact, chlamydial urethritis is the number one cause of first trimester pregnancy-related deaths in the United States.
- In males, chlamydia is characterized by painful urination and a discharge that is watery and copious.
- The discharge often is observed after urinating for the first time in the morning. Tingling sensations in the penis are generally evident.
- Inflammation of the epididymis can result in sterility, but this complication is uncommon.
- Chlamydial pharyngitis or inflammation of the anus (proctitis) is possible through oral or anal intercourse.
Treatment and Prevention
- Individuals who are asymptomatic remain infected.
- In symptomatic cases, the infection can be treated successfully (95% cure rate) with antibiotics.
- However, post-treatment rescreening is recommended to ensure reinfection has not occurred.
Reference and Sources
- https://projecttulip.org/internal-medicine/infectious-diseases/urogenital-system-infections/
- https://www.medicinenet.com/sexually_transmitted_diseases_stds_in_women/article.htm
- https://quizlet.com/206622057/microbiology-exam-4-flash-cards/
- https://www.studyblue.com/notes/note/n/13-16/deck/10753844
- https://cmr.asm.org/content/17/4/982
- https://www.scirp.org/Journal/PaperInformation.aspx?paperID=82383
- https://issuu.com/josemanuelvargas1/docs/emergency_medicine
Also Read:
- Fungal Disease
- what is microbiology?
- Types of microscopes
- The Genetic Code
- Microbial Fuel Cells
- Transposable Elements
- Measurements of microbial growth
- Different Types of chromatography
- Overview of lac operon an inducible operon
- Exposure and Transmission of Infectious Disease
- Standard Operating Procedures or SOP
- Carbohydrate: Structure, Functions and Types
- Electrophoresis: Overview, Principles and Types
- Granulocytes: Introduction, Types, Functions and Roles
- Fungi: Distribution, Morphology, Reproduction, Classification
- Histoplasmosis: Symptoms, Pathogenesis, Treatment and prevention
- Syphilis: Agent, Epidemiology, Symptoms, Treatment and prevention
