Leishmaniasis is a zoonosis disease caused by obligate intracellular parasites i.e., Leishmania spp.
It is usually transmitted from animal to humans or by the bite of infected female sandflies the parasites can transmit from human to human.
Different geographical areas have different species of Leishmania which are responsible for a variety of diseases ranging from :
Cutaneous Leishmaniasis
Mucocutaneous Leishmaniasis
Visceral Leishmaniasis ( Kala-azar)
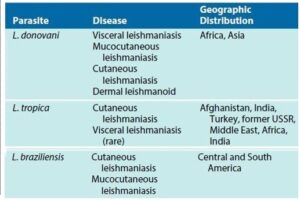
Three species of Leishmania are extensively studied i.e., L. donovani , L. tropica and L. brazilliensis.
Geographical distributions of Leishmania causing a range of diseases
Life Cycle of Leishmania
Usually, the life cycle of all Leishmania parasites is very similar despite their site of infection, clinical manifestations, and epidemiology.
The life cycle of Leishmania
During the life cycle, the parasite undergoes two stages: promastigote stage and amastigote stage.
In the promastigote stage, it appears as the long, slender form having a free flagellum, which exists in the saliva of the infected sandflies.
The amastigote stage takes place when the infected sandfly bites the human, injecting promastigotes that lose their flagella while entering the skin, which helps them to escape the host immune response.
The amastigote multiplies in reticuloendothelial cells, which cause ruptures in the cells, specific tissues ( cutaneous tissues, or visceral organs e.g., liver and spleen) destruction takes place.
As shown in the above figure, the amastigote stage is both diagnostic in humans and infectious stage in the sandflies.
The amastigote is ingested by sandflies and transforms into a promastigote, it multiplies in the fly midgut by binary fission.
The promastigote migrates to fly proboscis (mouthpart used for piercing to feed) after development, which can be introduced in humans while feeding.
The only exception in all life cycles of leishmaniasis is, in visceral leishmaniasis, throughout the body, infected reticuloendothelial cells can be found.
Epidemiology
Leishmania is transmitted in humans by adult female sandflies, belongs to the genera of Lutzomyia & Phlebotomus.
The natural reservoirs of the Leishmania are rodents, cats, dogs, sloths, etc.
The transmission of Leishmania is also seen by direct contact with infected wounds.
The geographical distribution of Cutaneous Leishmaniasis is observed in the Middle East regions such as Iran, Iraq, Syria, Saudi Arabia, and the core area in South America such as Brazil, Peru.
The occurrence of Mucocutaneous Leishmaniasis is mostly in Bolivia, Brazil, and Peru.
The most prevalent type in Asia is Visceral Leishmaniasis commonly known as Kala-Azar or dumdum fever in India, annually approx 500,000 new cases have been reported, commonly occur in Bangladesh, India, Nepal, Brazil and Sudan
The leishmaniasis infection can be endemic ( restricted to one place), epidemic (outbreak of the disease in the community), and sporadic ( occurring at irregular intervals at scattered places) and are usually zoonosis.
In India, black fever ( kala-azar) is anthroponosis i.e., transmission from human-vector-human, the post-dermal lesion of the kala-azar may be a reservoir that can be a cause of a spread in a community.
Clinical Manifestations
The type of Leishmaniasis infections depends on the species of Leishmania involved, HIV- related Leishmaniasis has also been reported caused by L.donovani in Africa and South Asia.
The initial sign of cutaneous leishmaniasis is commonly caused by L. tropica, a red papule (tiny red bump on the site of the fly’s bite) that appears in 2 weeks to 2 months after exposure.
The lesion becomes enlarged and ulcerated and it is intensely pruritic (itching).
The outer crust of the ulcer becomes hard and releases a serous substance which is thin watery exudates, this acts as a substrate for secondary infections which complicate the case, the lesion self recover without any treatment in few months but leaves rigid scars.
Mucocutaneous leishmaniasis initial symptoms and appearance of cutaneous ulcers is similar to the cutaneous leishmania, the only difference is destruction in mucous membranes and tissues are involved, 80% of untreated cases turns into mucocutaneous form because primary lesions are accompanied by the nasal and oral mucous spread of leishmania even after the lesion is healed.
Mucosal lesions don’t easily heal, and secondary infections are prevalent cause severe disfiguring facial form and occasionally fatal.
Visceral Leishmaniasis occurs sudden and severe, and it is fatal as it progresses slowly or can be asymptomatic, self recovering infections. The onset of symptoms such as fever, diarrhea, and anemia is gradual, and chill and sweating are common at the initial stage of infection, the incubation period may range from several weeks to a year.
The invasion and proliferation of the organisms in the reticuloendothelial system lead to the enlargement of visceral organs i.e., liver & spleen, weight loss, and loss of flesh occur; if glomeruli are infected, it may cause kidney damage.
The post-kala-azar dermal leishmaniasis occurs after the persistence of the disease, it appears as dark pigmented, regions of the skin consist of granuloma.
Diagnosis
Detection of amastigotes by smear stained of the sample obtained from the lesions or biopsy specimen. It is used for cutaneous and mucocutaneous leishmaniasis.
Giemma stained amastigote (L. donovani ) in touch preparation of the spleen
For visceral leishmaniasis, the specimen is obtained by splenic puncture, liver biopsy, lymph nodes aspirates. These specimen is examined under microscopy, and cultured.
Molecular detection is also used for the diagnosis, to detect nucleic acid (DNA or RNA) of Leishmania.
Detection of the antigens present in the urine sample is also helpful for the diagnosis of visceral leishmaniasis.
Treatment and Prevention
Currently, pentavalent carbohydrates- antimony compounds (sodium stibogluconate) such as Pentostam are used for the treatment of leishmaniasis.
For cutaneous leishmaniasis, standard therapy is used, in which antimony compounds are directly injected into the lesion.
There are several compounds that have shown their efficacy in the treatment of leishmania, those are fluconazole, miltefosine, other various formulations are amphotericin B, pentamidine.
Other than chemotherapy, heat, cryotherapy and surgical removal is done.
Due to an increase in drug resistance, pentavalent antimonials compounds have failed in the northern Bihar region of India, to overcome this situation four new therapies came into the existence:
Amphotericin B liposome formulations
Miltefosine (Oral )
Paromomycin ( Parenteral formulations)
Sitamaquine (Oral) i.e., 8- aminoquinolone
To control leishmania outbreak, its prevention involves:
Control of the reservoir host
Insect vector control by using repellents
Better treatment of human infections to avoid being a carrier