Botulism is an intoxication caused by neurotoxins produced by Clostridium botulinum, which adversely affects the synapses of the peripheral nervous system.
Botulinum is considered as most potent poison in the world.
Clinically, three types of manifestation of botulism are recognized – food-borne botulism, infant botulism, and wound botulism.
Etiology Agent
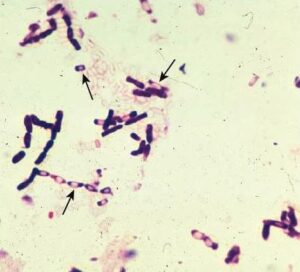
The etiology agent of botulism is Clostridium botulinum, a fastidious, anaerobic, and spore-forming rod.
Microscopic image of Clostridium
It is divided into four groups based on genetic and phenotypic properties.
Seven antigenic distinct botulinum toxins [A to G] have been recognized, basically, types A, B, E and F are associated with human diseases.
Other species of clostridia produce botulinum toxins, including C.butyricum [E- type], C. baratii [type F toxin], rarely associated with human disease, and C. argentinense [G- type toxin].
Pathogenicity and Virulence factors
Clostridium botulinum toxin is made up of 150,000 Da progenitor protein (A-B toxins).
Consists of a small subunit (light or A chain) with zinc- endopeptidase activity and large subunit B is nontoxic.
The toxin forms a complex with nontoxic proteins that protect neurotoxins during the passage through the digestive tract.
The carboxyl-terminal portion of the toxin, heavy chain interacts with specific sialic acid receptors along with glycoproteins present on the outer surface of motor neurons and triggers endocytosis of the toxin.
The neurotoxin remains at the neuromuscular junction, acidification of the endosome triggers the N- terminal, and heavy chain-mediated release of the light chain.
The botulinum endopeptidase inactivates the proteins that regulate the release of acetylcholine, by blocking the neurotransmission at peripheral cholinergic synapses.
In the normal function of nerve cells, a nerve impulse in the CNS causes vesicles filled with acetylcholine (ACh) to fuse with the neuron’s cytoplasmic membrane release of ACh into the synaptic cleft
Binding of ACh receptor of cell’s cytoplasmic membrane triggers the series of events that result in contraction of the muscle.
The botulinum toxin prevents the fusion of ACh to the neural cytoplasmic membrane which results in the clinical presentation of botulinum i.e., flaccid paralysis.
Mechanism of botulism toxin: [A] Normal Function at the neuromuscular junction [B] Botulinum toxin inhibits the fusion of ACh to the cell cytoplasmic membrane results in flaccid paralysis.
Epidemiology
C. botulinum is predominant in soil and water samples, A strains are found in the neutral and alkaline soil of the United States, B strains are found in the eastern part of organic soil, type E- strain is found in wet soil.
Three common forms of botulinum have been identified:
Food- bourne Botulinum
Annual cases reported is less than 30
Mostly consumption of home-canned food [include type A and B] cause symptoms
In rare cases, consumption of preserved fish [ include type E- toxin] may cause the botulinum
A small portion of intoxicated food can cause disease.
It usually starts 12- 36 hrs after consuming the toxin.
Later nerve dysfunction symptoms of botulinum like blurred vision, pupillary dilatation, and nystagmus, occur.
Paralysis begins with ocular, laryngeal, and respiratory muscles, later spread to the hand and legs.
The most serious symptom is respiratory paralysis.
The morality rate is 10- 20 %
Infant Botulism
Occur in infants between ages 3 weeks to 8 months.
Cases are less than 100 – annually
Food contaminated with botulinum spores-e.g., honey, milk powder.
When spores are consumed, multiples in the colon
Symptoms- constipation, poor muscle tone, and paralysis
Wound Botulism
Its rare, wound infection may cause C. botulinum to grow
C. botulinum produces toxins in a contaminated wound
Symptoms are identical to food- bourne botulinum
The incubation period is longer than 4 days.
Diagnosis
Diagnosed from blood samples, intestinal contents, or remaining food samples.
The test requires inoculation of mice also known as mouse bioassay,
In mouse bioassay, two aliquots are prepared, one mixed with antitoxin, inoculated intraperitoneal into the mice, if antitoxin protects the mice, toxin activity is confirmed.
Pre-heating treatment is done to remove all non- clostridia from the sample.
Enriched anaerobic media is used for culture; allow heat- resistance spores to germinate.
Treatment, Prevention, and Control
Patients with botulism require the following treatment measures:
Adequate ventilatory support to reduce mortality
Removal of the organisms from the gastrointestinal tract – via metronidazole or penicillin therapy.
Use of trivalent botulinum antitoxin vs A, B, and C to inactivate the toxins
Prevention is carried out by:
By destroying spores in food that is practically difficult
By maintaining the food in acidic pH or storage at 4˚C or colder.
By inactivating the preformed toxin by heating at 60˚ to 100˚ C for 10 mins.
For infant botulism, avoiding the consumption of honey by infants.