
Introduction
Helicobacter pylori (H. pylori) is a Gram-negative, spiral-shaped, microaerophilic bacterium that colonizes the gastric mucosa of humans. It is one of the most widespread chronic bacterial infections globally, affecting more than half of the world’s population. Despite its small size, H. pylori is medically significant due to its strong association with peptic ulcer disease, chronic gastritis, mucosa-associated lymphoid tissue (MALT) lymphoma, and gastric adenocarcinoma. The World Health Organization (WHO) classifies H. pylori as a Group I carcinogen, making its study crucial for public health and clinical microbiology.
Understanding its morphology, virulence factors, disease mechanisms, and diagnosis helps guide effective treatment and prevention strategies, especially amid rising antibiotic resistance.
Taxonomy and Classification
| Taxonomic Rank | Classification |
| Domain | Bacteria |
| Phylum | Proteobacteria |
| Class | Epsilonproteobacteria |
| Order | Campylobacterales |
| Family | Helicobacteraceae |
| Genus | Helicobacter |
| Species | Helicobacter pylori |
Morphology and Structural Characteristics
Helicobacter pylori exhibits several unique structural and biochemical characteristics that allow it to survive the harsh gastric environment.
Key Morphological Features:
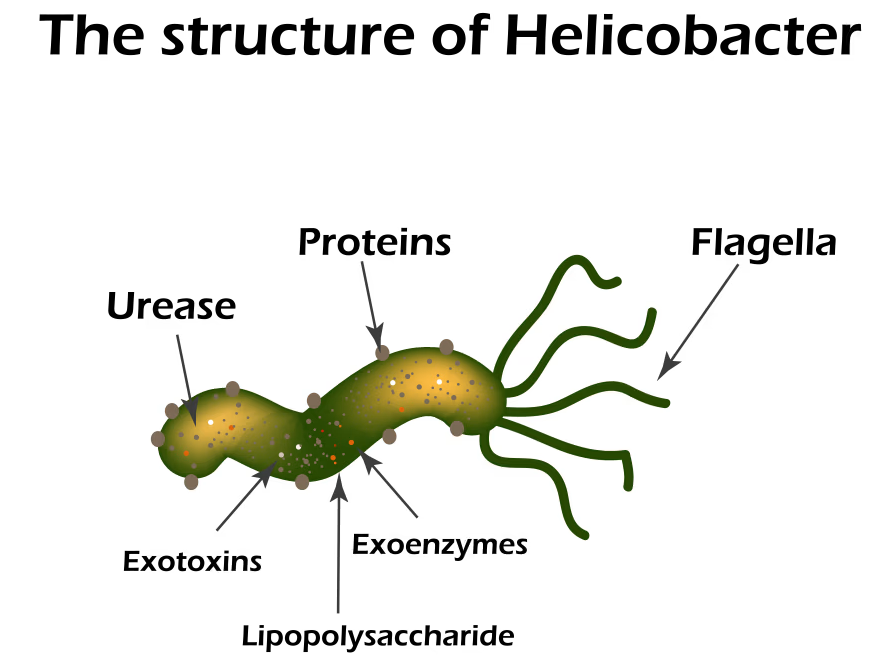
- Shape: Spiral or curved rods with 2–6 unipolar sheathed flagella.
- Size: 2.5–4.0 µm long × 0.5–1.0 µm wide.
- Gram Reaction: Gram-negative.
- Spores: Non-spore-forming.
- Capsule: Absent, but surrounded by a typical Gram-negative outer membrane.
- Motility: Highly motile due to polar flagella, allowing movement through viscous gastric mucus.
- Oxygen Requirement: Microaerophilic (optimal O₂ concentration 5–10%).
Unique Survival Feature:
Strong Urease Production: Converts urea into ammonia and carbon dioxide, forming a protective alkaline microenvironment. This is essential for survival in acidic gastric pH (~2).
Growth and Cultural Characteristics
Optimal Growth Conditions:
- Atmosphere: Microaerophilic (5% O₂, 10% CO₂, 85% N₂).
- Temperature: 37°C (human body temperature).
- pH Range: Optimal pH 6.5–7.5, though urease allows survival at low pH.
Culture Media:
- Selective Media: Skirrow’s medium, Columbia agar, and chocolate agar enriched with blood or serum.
- Colony Appearance: Small, translucent, dew-drop-like colonies visible after 3–5 days.
Biochemical Reactions:
- Urease: Positive (major diagnostic marker)
- Catalase: Positive
- Oxidase: Positive
- Nitrate Reduction: Positive
- Indole: Negative
Epidemiology and Habitat
H. pylori primarily colonizes the gastric antrum but can also be found in the fundus and duodenum.
Key Epidemiological Facts:
- Over 50% of the global population is infected.
- Higher prevalence in developing countries due to:
- Poor sanitation
- Overcrowding
- Unsafe water and food sources
Transmission Routes:
- Oral–oral
- Fecal–oral
- Gastric–oral (vomit contact)
Most infections occur during childhood and persist lifelong if untreated.
Virulence Factors of Helicobacter pylori
Several virulence factors contribute to colonization, immune evasion, tissue damage, and carcinogenesis.
- Enzyme Ureas: Transforms urea into ammonia and carbon dioxide, which neutralizes stomach acid and establishes a local alkaline microenvironment for survival.
- Motility and Flagella: Facilitates epithelial surface colonization and movement via the thick gastric mucus.
- Adhesins: The outer membrane proteins BabA (Blood group antigen-binding adhesin) and SabA (Sialic acid-binding adhesin) help with epithelial cell adhesion.
- Cag Pathogenicity Island (CagA): Encodes a type IV secretion system that introduces the CagA protein into the epithelial cells of the host. CagA promotes inflammation, alters the cytoskeleton, interferes with cellular signaling, and raises the risk of cancer.
- Vacuolating Cytotoxin A (VacA): Induces apoptosis, modulates the immune response, and causes vacuolation in gastric epithelial cells (the creation of big vacuoles).
- Lipopolysaccharide (LPS) and lipoproteins: Less endotoxic activity than other Gram-negative bacteria, but it aids in immune evasion and persistent inflammation.
- Superoxide Dismutase (SOD) and Catalase: Safeguards the bacteria from oxidative injury caused by the host immune system.
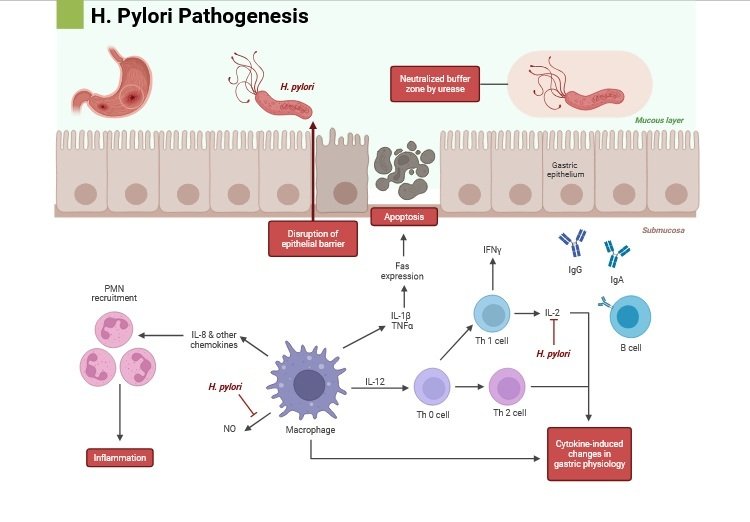
Pathogenesis of H. pylori Infection
The disease progression involves five major stages:
- Colonization Phase: The flagella help H. pylori get past the mucus layer and reach the epithelial surface after it enters the stomach. By counteracting acidity in the immediate area, urease aids in survival.
- Adhesion to Gastric Cells: By attaching to epithelial receptors in a precise manner, adhesins facilitate colonization.
- Inflammation and Tissue Damage: VacA and CagA both cause epithelial integrity to break down and trigger an inflammatory reaction. Neutrophils and lymphocytes are attracted by the release of cytokines such as IL-8, which results in tissue damage.
- Ulcer Formation and Persistent Gastritis: Continued inflammation causes ulcer formation in the stomach or duodenum over time by eroding the mucosa and depleting the protective mucus.
- Carcinogenesis: Chronic infection can lead to dysplasia, intestinal metaplasia, atrophic gastritis, and eventually stomach adenocarcinoma. The World Health Organization (WHO) lists H. pylori as a Group 1 carcinogen.
Clinical Manifestations
Many infected individuals remain asymptomatic, but symptomatic cases may present with:
Gastrointestinal Conditions:
- Chronic gastritis
- Peptic ulcer disease (PUD)
- Duodenal ulcers
- Gastric adenocarcinoma
- MALT lymphoma
Common Symptoms:
- Epigastric pain/burning (worse on empty stomach)
- Bloating and frequent burping
- Early satiety
- Loss of appetite
- Nausea or vomiting
- Unexplained weight loss

Diagnosis of Helicobacter pylori
Diagnosis includes both non-invasive and invasive methods.
Non-Invasive Tests
- Urea Breath Test: The patient eats urea that has been marked with the carbon isotope (¹³C or ¹⁴C). In exhaled breath, labeled CO2, which is produced by the action of the urease of H. pylori, can be found. Very precise and responsive.
- Stool Antigen Test: Recognizes bacterial antigens in feces, making it helpful for diagnosis and verification following treatment.
- Serological Test: Detects anti-H. pylori antibodies, which suggests exposure but does not always mean an active infection.
Invasive Tests (Endoscopy-Based)
- Rapid Urease Test (CLO Test): A gastric biopsy sample is placed in urea-containing media with a pH indicator; a change in color indicates urease activity.
- Histology: Biopsy examined with stains such as:
- Giemsa
- Warthin-Starry
- Immunohistochemistry
- Culture: The biopsy sample was cultured under microaerophilic conditions in order to isolate bacteria and assess antibiotic susceptibility.
- PCR: Detects specific DNA sequences of H. pylori and resistance genes (e.g., mutations in 23S rRNA).
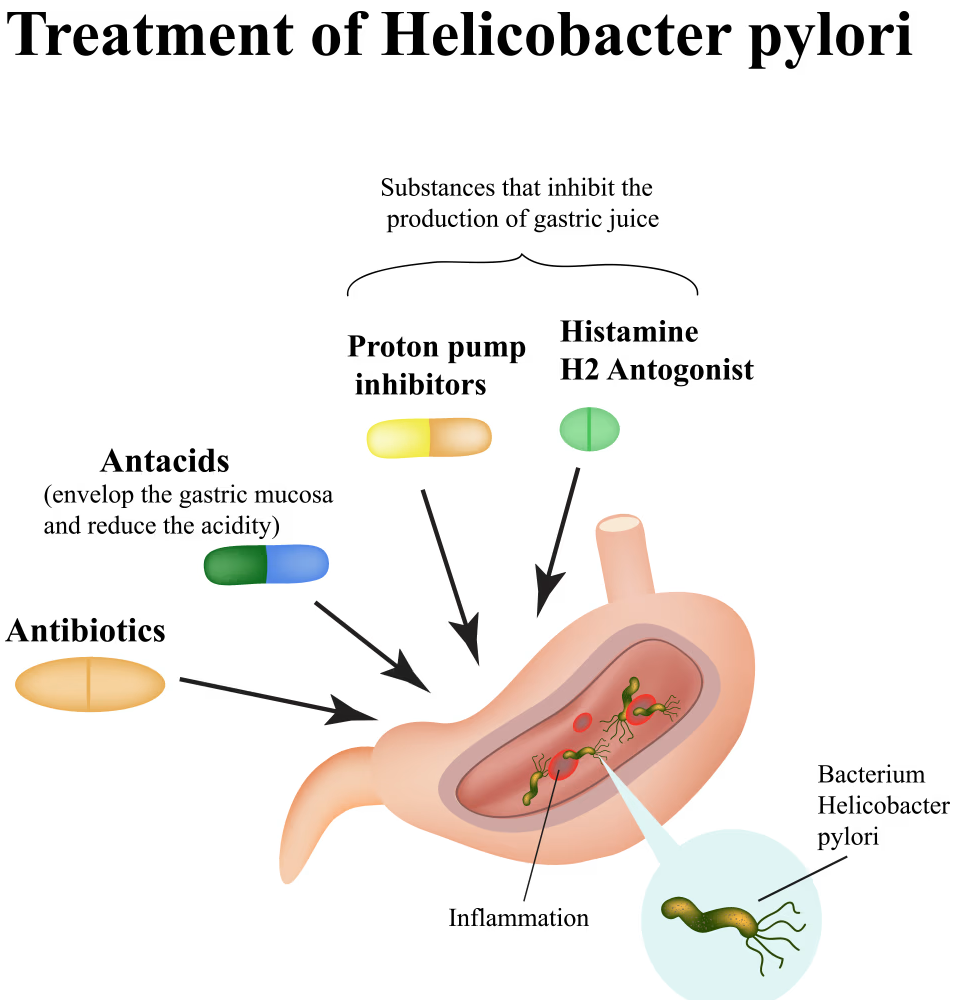
Treatment of H. pylori Infection
Treatment regimens must be tailored regionally as a result of growing antibiotic resistance. The main goal is complete elimination.
- First-Line Therapy:
- Ten to fourteen days of triple therapy.
- Amoxicillin + Clarithromycin + Proton Pump Inhibitor (PPI).
- Alternative / Quadruple Therapy:
- The Quadruple Therapy based on Bismuth.
- Metronidazole, tetracycline, bismuth subsalicylate, and PPI.
- Sequential or Concomitant Therapy:
- To combat resistance, many antibiotics are combined in phased regimens.
- Resistance Considerations:
- The world is seeing an increase in resistance to clarithromycin, metronidazole, and levofloxacin.
- Molecular identification of resistance genes or culture-guided therapy increases the likelihood of success.
- Adjunctive Therapy:
- Probiotics have the potential to lower adverse effects and raise eradication rates.
- By decreasing the acidity in the stomach, PPIs boost the effectiveness of antibiotics.
- Confirmation of Eradication:
- Four to six weeks after treatment, a urea breath or stool antigen test was administered.
Prevention and Control
Although no vaccine exists, preventive strategies include:
- Maintaining proper hygiene.
- Drinking clean, safe water.
- Proper food handling.
- Avoiding sharing utensils.
- Screening individuals with family history of gastric cancer or ulcer disease.
Complications of H. pylori Infection
Untreated chronic infection can lead to:
- Peptic ulcer
- Gastric atrophy
- Intestinal metaplasia
- Dysplasia
- Gastric adenocarcinoma
- MALT lymphoma
- Iron deficiency anemia
- Idiopathic thrombocytopenic purpura (ITP)
Conclusion
Helicobacter pylori is a globally prevalent pathogen capable of surviving the harsh gastric environment through powerful virulence mechanisms such as urease production, flagellar motility, and cytotoxins like CagA and VacA. It plays a major role in chronic gastritis, peptic ulcer disease, MALT lymphoma, and gastric cancer. Early diagnosis, appropriate antibiotic therapy, and confirmation of eradication are essential for preventing long-term complications. With rising antibiotic resistance, tailored therapy—guided by susceptibility tests—has become increasingly important. Maintaining good hygiene, safe food handling, and public awareness can significantly reduce infection rates and associated health burdens.
Also Read:
- https://microbiologynotes.org/immunoglobulin-introduction-structure-and-function/
- https://microbiologynotes.org/antimicrobial-chemotherapy-history-characteristics-and-tests/
- https://microbiologynotes.org/trichoderma-overview-mechanism-of-action-and-applications/
- https://microbiologynotes.org/cancer-intro-types-development-and-therapy/
- https://microbiologynotes.org/anti-protozoan-drugs/
Reference and Sources
- https://www.mayoclinic.org/diseases-conditions/h-pylori/symptoms-causes/syc-20356171
- https://my.clevelandclinic.org/health/diseases/21463-h-pylori-infection
- https://www.medicoverhospitals.in/diseases/helicobacter-pylori-infection/
