Shigella – Epidemiology, Pathogenesis, and Treatment
Introduction
Shigella is classified among the class of Enterobacteriaceae, more related to E.coli.
It’s a gram-negative rod, non-motile and unlike E.colidoesn’t involve gas formation while glucose fermentation, and is not capable of fermenting lactose.
Antigenic makeup is also similar to the E.coli with an exception of the absence of flagella and H antigen.
The genus Shigella is mainly divided into four serogroups on the basis of specific O antigens organization and biochemical reactions:
Serogroup A- Shigella dysenteriae
Serogroup B- Shigella flexneri
Serogroup C- Shigella boydii
Serogroup D- Shigella sonnei
Further serogroup D i.e., Shigella sonnei is subdivided on the basis of the O antigen into 38 serotypes.
Shigella is an invasive pathogen, capable of invading and multiplying within a wide variety of epithelial cells, especially enterocytes.
The first discovered Shigella species was S. dysenteriae type A1 (Shiga Bacillus), which is the highest producer of the Shiga toxin, other species produce several molecular forms of Shiga toxins.
Epidemiology
Shigella is an etiologic agent of Shigellosis, and the disease is confined to humans with no animal reservoir.
Over 30 years in the U.S, the reported number of cases ranged between 8- 12 per 100,000 populations.
It is considered as the prevalent cause of infectious diarrhea, in many countries, mortality per year is approx 600,000.
The transmission mode is a fecal-oral route through person-to-person contact, also spread by food & water contamination.
The dose of infection is less than 200 microorganisms; therefore the mode of spread is efficient, the secondary attack is 40% higher.
The major spread of Shigellosis is related to community and personal sanitary practices.
The disease is widespread where sanitary practices and poor hygienic conditions are inadequate, most developed countries are affected and also prevalent in the places affected by natural disasters and war.
In underdeveloped tropical, the most common Shigella species are S.dysenteriae, S. flexneri, and S. sonnei. The most severe disease form of dysentery i.e., Bacillary dysentery is caused by S. dysenteriae, type 1.
Pathogenesis
Shigella strains are acid-resistant because of that it survives the stomach passage to extend in the intestines.
The event of the pathogenesis of Shigella includes invasion of the mucosa of the colon.
Triggers the response of acute inflammatory, which causes ulcer in the mucosa and forms the abscess.
Invasion and spread are followed in the multistep process:
Step 1:
Schematic representation of invasion of Shigella in the M cells
Shigella cross the mucosal membrane by M cells located in the Peyer’s patches, which is related to the follicle of the intestines, which is devoid of a highly organized absorptive layer of enterocytes.
Attachment of the bacteria leads to modification of the cytoskeleton in which process involves filamentous actin accumulation underneath the cytoplasmic membrane of the host cell, which induces the engulfment and internalization of the bacterium Shigella into the host cell by endocytosis.
The adherence is selective to the M cells and it is transcytosed through them, into the underlying phagocytic cells which cause apoptosis, in which IL-1β is, released which results in the draw the polymorphonuclear leukocytes towards the infected tissues.
Microscopic image of Shigella invading M cells, attracting the macrophages underlying within the M cells
This process destabilized the intestinal wall integrity, which allows bacteria to reach the deeper epithelial cells.
Step 2
Shigella bacterium push the basolateral membrane of enterocytes to invade the adjacent cell and movement is gained by actin polymerization
Bacteria are released from the M cells and make contact with the basolateral side of the enterocytes and again multistep invasion process is mediated by the set of the invasion plasmid antigens which includes IpaA, IpaB, and IpaC.
While in contact, antigens are injected into the enterocyte by the type III secretion system, and each antigen has its specific actions.
These actions include cell attachment, actin polymerization, reorganization of the cytoskeleton.
Step 3:
Bacteria invading adjacent cells and multiplying in the M cell
Shigella is highly adaptive to intracellular conditions and uniquely uses it to continue the course of the infection.
They tend to escape the phagocytic vacuole, within 15 minutes and enter the cytoplasm of the host cell.
Instantly, they orient alignment with the actin filaments of the cytoskeleton and start the process in which they control the actin polymerization, this helps to create actin tails at the end of the bacterium which assists the movement through cytoplasm also help to replicate in the cell.
Finally, bacteria come across the host cell membrane which is adjacent to the neighboring enterocytes; they push the membrane about 20µm into the adjacent cell, which leads to invasion into the neighboring cell that appears like a finger-like projection.
Eventually, projection pinch-off, and the bacterium is placed within the new cell, enclosed in the double membrane, which is lysed and the free bacterium is released in the cytoplasm to continue the fresh cycle.
The radial stretching or expansion of the cell during the pathogenesis of the bacteria forms focal mucosal ulcers of the colon.
Because of the ulcers, the hemorrhagic component is added and an intense acute inflammatory response is evoked when bacteria reach the lamina propria (thin layers of the connective tissue), usually, infection is not extended beyond the lamina.
In this case, diarrhea caused by the process is majorly inflammatory, consists of a small volume of stool consist of RBCs, WBCs, and bacteria. It is called classic dysentery.
dysentery strains of Shigella produce exotoxins like Shiga toxin, which has one A subunit and five B subunits.
The B subunits bind with glycolipid (Gb3) present in the host cell and promote the transfers of the A subunit into the cell.
The A subunit functions to cleave the 28S rRNA in the 60S ribosomal subunit, which prevents the binding of the aminoacyl in RNA transfer and disrupts the synthesis of the proteins.
The combined action of toxin subunits damages the epithelial cells of the intestines, in the rare case of some patients, Shiga toxin can damage the glomerular endothelial cells, which causes renal failure.
Clinical Symptoms
As Shigella causes acute inflammatory colitis & bloody diarrhea, so major symptoms are characterized are of dysentery syndrome.
The clinical symptoms appear in 1 to 3 days after ingestion of bacteria, initial colonization of bacteria occurs in the small intestine and multiply within 12 hrs
It includes abdominal cramps, tenesmus i.e., painful strain while passing the stools, frequent and small volume, bloody mucous discharge.
S. sonnei generally causes watery diarrhea, followed by the symptoms like fever, anorexia (loss of appetite), malaise (general feeling of unease or discomfort), and occasionally myalgia (muscles pain). Later, diarrhea may turn bloody.
The symptoms get severe when S. flexneri is involved.
Most severe symptoms are observed with S. dysenteriae infection.
The broad majority of Shigellosis cases are resolved after 2- 5 days; the mortality rate of Shiga toxin caused dysentery is high as 20%.
Diagnosis
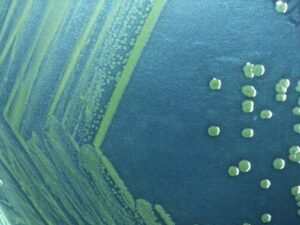
The selective media such as Hektoen enteric agar is used to isolate all Shigella strains, these media contains inhibitory chemical additives to prevent the growth of the facultative flora (e.g., E. Coli, Klebsiella). Usually, stool samples from patients are cultured.
Colony characteristics of Shigella on Hektoen Enteric agar appear as green moist transparent colonies.
Colony characteristics of Shigella sonnie on Hentoen enteric agar
It also contains indicators such as bromothymol blue, acid fuchsin, and ferric iron which is utilize classic biochemical reactions to confirm the presence of the Shigella colonies.
The diagnosis in most of the patients, is performed on the basis of the fresh blood present in the stool samples, neutrophils in the fecal smears are detected by microscopic examination which strongly suggests the sign of Shigellosis.
For confirmation tests, slide agglutination tests using specific O group antisera (A, B, C, and D), confirm the strains of the Shigella.
Treatment
Most of the antimicrobial agents are efficient in the treatment of Shigellosis because it is considered self-limiting (self recovering), but treatment is beneficial in shortening the period of the illness.
Previously ampicillin was used, but due to an increase in resistance rate of 5-50%, it is changed to TWP-SWX in most of the area.
Recently, quinolones and cephalosporins of the third generation have been used.
Prevention
To prevent the spread of Shigellosis, community standard sanitation practices like water chlorination and sewage disposal should be considered.
Good personal sanitation practices should be maintained such as handwashing & proper cooking of the food.