
Klebsiella
Introduction
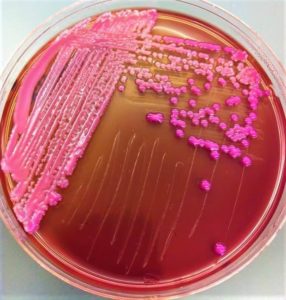
Klebsiella are gram-negative, nonsporing, non-motile bacilli that grow well on ordinary media, produce pink mucoid colonies on MacConkey’s agar. They are usually found in the intestinal tract of humans and animals or free living in soil, water, and on plants.
Classification
Their classification has undergone various modifications. The name K. pneumoniae is used for the species as a whole. It is further divided into 4 subspecies. The most frequently encountered, biochemically typical form of it is known as K. pneumoniae subsp. aerogenes, K. pneumoniae subsp. ozaenae, K. pneumoniae subsp. pneumoniae, K. pneumoniae subsp. rhinoscleromatis. Indole-producing strains that resemble K. pneumoniae subsp. aerogenes biochemically are classified in a separate species, K. oxytoca.
Morphology
They are short, plump, gram-negative, non-sporing, capsulated, non-motile bacilli, 1–2 μm long and 0.5–0.8 μm wide with parallel or bulging sides and slightly pointed or rounded ends.
Cultural Characteristics
Klebsiellae grow well on ordinary media at a temperatures between 12°C and 43°C (optimum, 37°C) in 18–24 hours. On MacConkey agar, the colonies typically appear large, mucoid and red in colour. Mucoid nature of colonies is due to capsular material produced by the organism.
Biochemical Reactions
They ferment sugars (glucose, lactose, sucrose, mannitol) with production of acid and gas. They are urease positive, indole negative, MR negative, VP positive and citrate positive (IMViC – – ++). These reactions are typical of K. pneumoniae subsp. aerogenes.
Antigenic Structure
Klebsiella possess capsular (K) and somatic(O) antigens.
- Capsular (K) antigen: On the basis of capsular (K) antigens, the klebsiellae have been differentiated, into 80 serotypes. Members of capsular types 1–6 occur most frequently in the human respiratory tract.
Capsular antigens are usually detected by means of the capsular ‘swelling’ reaction, counter current immunoelectrophoresis and enzyme-linked immunosorbent-assay (ELISA).
- Somatic (O) antigen: Five different somatic or O antigens (01–05) occur in various combinations with the capsular antigens. Four of the five Klebsiella O antigens are identical to or related to E. coli O antigens.
Typing Methods
- Bacteriocin (Klebocin or pneumocin) typing
- Phage typing
- Biotyping
- Resistotyping
- Molecular typing methods:
- Plasmid analysis
- DNA profiling by random amplified polymorphic
- DNA (RAPD) and pulsed-field gel electrophoresis
Pathogenicity
Klebsiella pneumoniae can cause a primary community-acquired pnuemonia, nosocomial infections, urinary tract infections, wound infections, bacteremia and meningitis and rarely diarrhea. In some hospital, K. pneumoniae has replaced E. coli as the leading blood culture isolate. As most strains are resistant to antibiotics, treatment poses serious problems.
Pneumonia
Klebsiella pneumonia is a serious disease with high case fatality. The typical patient is a middle- or older-aged man who have medical problems. Positive blood cultures can be obtained in about 25% of the cases.
Diarrhea
Some strains of K. pneumoniae isolated from cases of diarrhea have been shown to produce an enterotoxin very similar to the heat stable toxin of E. coli.
K. ozaenae is a bacillus associated with ozena, an uncommon, chronic disease in which there is atrophy of the nasal mucosa characterized by foul smelling nasal discharge.
K. rhinoscleromatis causes rhinoscleroma, a chronic granulomatous hypertrophy of the nose. K. oxytoca may be rarely isolated from clinical specimens.
Distinguishing reactions of Klebsiella species
| Tests | K. pneumoniae subspecies | K oxytoca | |||
| aerogenes | pneumoniae | ozaenae | rhinoscleromatis | ||
| Gas from glucose | + | + | V | – | + |
| Acid from lactose | + | + | V | – | + |
| Urease | + | + | V | – | + |
| Citrate | + | + | V | – | + |
| Malonate | + | + | – | + | + |
| MR | – | + | + | + | V |
| VP | + | – | – | – | V |
| Lysine decarboxylase |
+ | + | V | – | + |
| KCN | + | + | + | ± | + |
| V= Variable | |||||
Laboratory Diagnosis
Diagnosis is made by culturing appropriate specimens on blood agar and Mac Conkey agar and identifying the isolate by biochemical reactions. Antibiotic sensitivity should invariably be done. Many strains carry plasmids determining multiple drug resistance.
Klebsiella pneumoniae treatment
They are normally susceptible to cephaloporins, especially β-lactamase stable derivatives such as cefuroxime and cefotaxime, and to fluoroquinolones. They are often sensitive to gentamicin and other aminoglycosides., but
transferable enzymic resistance to aminoglycosides and other antimicrobial agents has become common in strains found in some hospitals.
Klebsiella infection of the urine often responds to trimethoprim, nitrofurantoin, co-amoxiclav or oral cephalosporins. Pneumonia and other serious infections require vigorous treatment with aminoglycoside or a cephalosporin, such as cefotaxime.
Reference and Sources
- https://tspbi.bcrc.firdi.org.tw/BSAS_RI_articles.jsp?BCRCID=10692&source=uniprot
- https://eazzynotes.com/klebsiella/
- https://universe84a.com/collection/klebsiella-pneumoniae/
- https://www.sciencedirect.com/topics/immunology-and-microbiology/raoultella
- https://solange-george.com/microbiology-practicals/preparation-macconkey-agar-medium-mac-principlecomposition/medical-paramedical-studynotesggq79m4933ma-s-u
- http://priede.bf.lu.lv/grozs/Mikrobiologijas/Mediciniska_mikrobiol/E.coli.doc
Also Read:
- E.coli-Epidemiology, Pathogenesis and Treatment
- Immunoglobulin: Introduction, Structure and function
- Microbial Identification and Strain Typing Using Molecular Techniques
- Virology: Introduction, Virus classification and Viral diseases
- Omicron: Introduction, Scientist vs Omicron and Vaccines for omicron
- Pseudomonas aeruginosa-Etiology, Pathogenesis and Treatment
- https://microbiologynotes.org/pneumocystis-pneumonia-symptoms-causative-agent-pathogenesis-treatment-and-prevention/